Visual Diet and Ocular Health.
Bridge the critical data gap between episodic clinical visits and real-world patient behavior. Blink® Frames provide continuous, high-fidelity monitoring of the environmental and behavioral risk factors driving myopia progression.
The Global Burden of Refractive Error and Axial Elongation
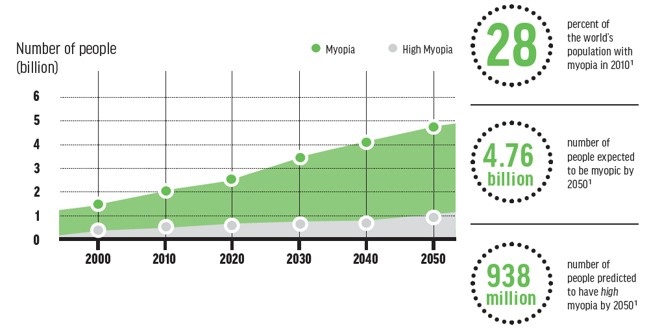
The 21st century has witnessed a fundamental shift in ocular development patterns, driven by rapid urbanization, educational intensification, and digitalization. As shown on the graphic below, current predictive modeling suggests that by the year 2050, an estimated 4.76 billion people will be myopic, with 938 million projected to suffer from high myopia (Holden et al., 2016). High myopia drastically increases the risk of irreversible vision loss, raising the risk of Glaucoma by 14x, Retinal Detachment by 22x, and Myopic Macular Degeneration by 41x (Flitcroft, 2012).
While the standard of care has evolved from passive correction to active management—utilizing optical and pharmaceutical inhibition of growth—the execution of these strategies remains fundamentally reactive. Clinicians measure axial length and refraction at discrete intervals, often 6 to 12 months apart, creating a clinical "blind spot" where irreversible elongation can occur before intervention is intensified. Practitioners currently rely on subjective anamnesis and parental reporting to assess compliance and environmental risk factors, methodologies fraught with recall bias and inaccuracy.
The Protective Mechanism of Outdoor Illuminance
The most robust environmental association found in modern myopia research is the protective effect of time spent outdoors (Dhakal et al., 2022). Emmetropization is regulated by the visual feedback of the retina, and the leading hypothesis for this protective effect is the "light-dopamine" mechanism (Liu et al., 2023).
Exposure to high-intensity ambient light stimulates the release of dopamine from retinal dopaminergic amacrine cells, which acts as a paracrine stop-signal for axial elongation, likely by inhibiting scleral remodeling (Cohen et al., 2012; Troilo et al., 2019). Daylight activates the photopigment melanopsin, which is localized in the axon membranes of intrinsically photosensitive retinal ganglion cells (ipRGCs); this activation increases the release of dopamine via an excitatory synaptic contact to dopaminergic amacrine cells (Amorim-de-Sousa et al., 2024).
Evidence shows that indoor environments—even those perceived as well-lit—consistently fail to reach the intensities required for myopia protection. Typical indoor settings rarely reach 500 lux, providing insufficient stimulation to the retinal pathways that regulate eye growth (Wen et al., 2020; Bhandary et al., 2021). While researchers have historically relied on a static 1,000-lux threshold as a proxy for outdoor time, this binary "on/off" measurement fails to account for the varying spectral composition and biological potency of natural light. To close this gap, we at Blink® have developed a time-compensated model (Rickard et al., 2026) that moves beyond basic sensors. While static models often ignore beneficial exposure during "golden hours" because they don't hit an arbitrary 1,000-lux ceiling, our dynamic algorithm accounts for the cumulative dose of light. By weighing intensity against duration, Blink® captures the subtle but biologically significant dawn and dusk periods giving your eye doctor a complete and accurate record of the light that shapes your child's vision for life.
Digital Screen Time and Myopigenic Acceleration
The counterpart to the lack of outdoor light is the intensification of near-work demands. A 2025 systematic review and dose-response meta-analysis demonstrated that each additional hour of daily digital screen time increases the odds of myopia by 21% (OR 1.21; 95% CI 1.13-1.30) (Ha et al., 2025).
Notably, the risk exhibits a sigmoidal pattern. The dose-response curve indicates that the odds of myopia start to increase significantly with daily screen time of more than 1 hour, jumping from an odds ratio of 1.05 at 1 hour to 1.97 at 4 hours of daily exposure (Ha et al., 2025). Beyond 4 hours per day, the rate of odds increase slows, revealing a sigmoidal pattern (Ha et al., 2025).
"The interplay between these factors—light exposure acting as a 'brake' and near work acting as an 'accelerator'—determines the refractive trajectory of the pediatric eye. Without objective measurement, we are navigating the myopia epidemic blindfolded." - Dr. Jonathan Li
Isolating Non-Responders from the Non-Compliant
Breakthrough lens technologies offer a powerful defense against myopia. However, their biological success depends on a critical factor: consistent, full-time wear (Logan and Bullimore, 2024). Compared to single vision lenses, H.A.L.T. (Highly Aspherical Lenslet Target) specialized lenses slowed myopia progression by 71% on average over 2 years (clinical trial data, www.essilor.com). Recent studies indicate that Defocus Incorporated Multiple Segments (DIMS) lenses can successfully slow axial length progression to 0.16 ± 0.2 mm/year (Jethani, 2024). Since the efficacy of optical interventions relies on the eye receiving a specific optical signal (eg. myopic defocus) for a significant portion of the day, there is an unmet clinical need for accurate daily frame wear time data.
If a child shows rapid axial elongation despite a therapeutic prescription, the clinician faces a diagnostic dilemma: is it a physiological failure, or a compliance failure? By objectively verifying spectacle wear-time, Blink® Frames ensure physiological treatment protocols are met, allowing the clinician to differentiate between a true non-responder and a non-compliant patient.
Objective Ocular Health via Blink® Frames
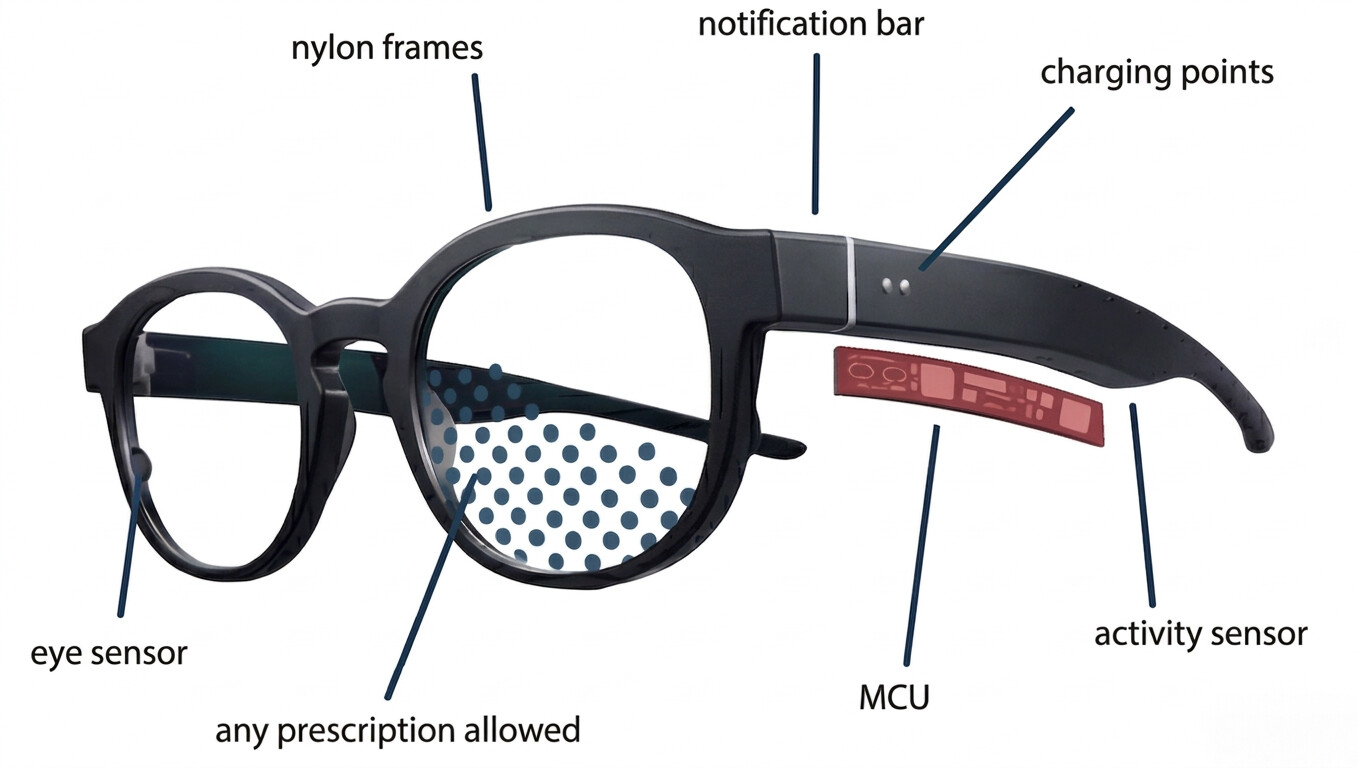
Blink® Frames (Globe Biomedical, Riverside, CA) are an FDA Registered medical device that integrates into a lightweight 16g form factor. Utilizing proprietary inward-facing micro-cameras and multi-sensor arrays powered by on-device AI, the platform passively captures over 250,000 sensor data points and 4,000 ocular images per user, per day.
- Clinical Validation: In collaboration with UCSF and UCI clinicians, a cross-sectional study was presented at the International Myopia Conference. In this study, researchers validated the Blink® Frames’ ability to continuously measure illuminance along the line of sight using chromatic spectral composition analysis (Li et al., 2024).
- Unmatched Accuracy: The 2024 validation data demonstrated >96% accuracy in frame wear-time detection, >94% accuracy in patch-wear adherence, and >93% accuracy in outdoor-time detection.
- Privacy-First Design: Unlike consumer smart glasses, the sensors are strictly inward-facing, observing the eye itself continuously and passively without recording the external world.
Ready to offer Blink® Frames at your practice?
Register your interest now and be first in your territory when onboarding opens.
References
- Flitcroft, D. I. (2012). The complex interactions of retinal, optical and environmental factors in myopia aetiology. Progress in Retinal and Eye Research, 31(6), 622-660.
- Wen, L., Cao, Y., Cheng, Q., et al. (2020). Objectively measured near work, outdoor exposure and myopia in children. British Journal of Ophthalmology, 104(11), 1542-1547.
- Troilo, D., Smith, E. L., Nickla, D. L., et al. (2019). IMI - Report on Experimental Models of Emmetropization and Myopia. Investigative Ophthalmology & Visual Science, 60(3), M31-M88.
- Holden, B. A., Fricke, T. R., Wilson, D. A., et al. (2016). Global prevalence of myopia and high myopia and temporal trends from 2000 through 2050. Ophthalmology, 123(5), 1036-1042.
- Ha, A., Lee, Y. J., Lee, M., Shim, S. R., & Kim, Y. K. (2025). Digital Screen Time and Myopia: A Systematic Review and Dose-Response Meta-Analysis. JAMA Network Open, 8(2), e2460026.
- Li, J., Park, J., Rickard, M., Suitt, D., Suh, D., Hakimeh, C., Ahmed, R. (2024). Validation of novel smart frames as a device for measuring outdoor time and illuminance. Presented at the 19th International Myopia Conference, Hainan, China.
- Jethani, J. (2024). Effect of defocus incorporated multiple segments lenses on halting myopia progression not responding to low-concentration atropine (0.01%) eye drops. Indian Journal of Ophthalmology, 72(Suppl 4), S709-S711.
- Logan, N. S., & Bullimore, M. A. (2024). Optical interventions for myopia control. Eye, 38(3), 455-463.
- Essilor (www.essilor.com) — Results from a prospective, randomized, double-masked, multicenter U.S. clinical trial in myopic children aged 6–12 years at initiation of treatment.
- Amorim-de-Sousa, A., Chakraborty, R., Collins, M. J., et al. (2024). Blue light stimulation of the blind spot in human: from melanopsin to clinically relevant biomarkers of myopia. Bioelectronic Medicine, 10:26.
- Dhakal, R., Shah, R., Huntjens, B., Verkicharla, P. K., & Lawrenson, J. G. (2022). Time spent outdoors as an intervention for myopia prevention and control in children: an overview of systematic reviews. Ophthalmic and Physiological Optics, 42(3), 545-558.
- Liu, X., Wang, P., Xie, Z., et al. (2023). One-year myopia control efficacy of cylindrical annular refractive element spectacle lenses. Acta Ophthalmologica, 101, 651-657.
- Rickard, M. J., Park, J., Sears, J., Suitt, D., Reardon, A., Ringenberg, R., and Li, J. A Dynamic, Time-Dependent Lux Threshold Algorithm for Quantifying Outdoor Time with Myopia Wearables. Accepted for podium presentation at the Annual Meeting of the Association for Research in Vision and Ophthalmology (ARVO), Denver, CO, May 2026.
- Bhandary, S. K., Dhakal, R., Sanghavi, V., & Verkicharla, P. K. (2021). Ambient light level varies with different locations and environmental conditions: Potential to impact myopia. Plos one, 16(7), e0254027